
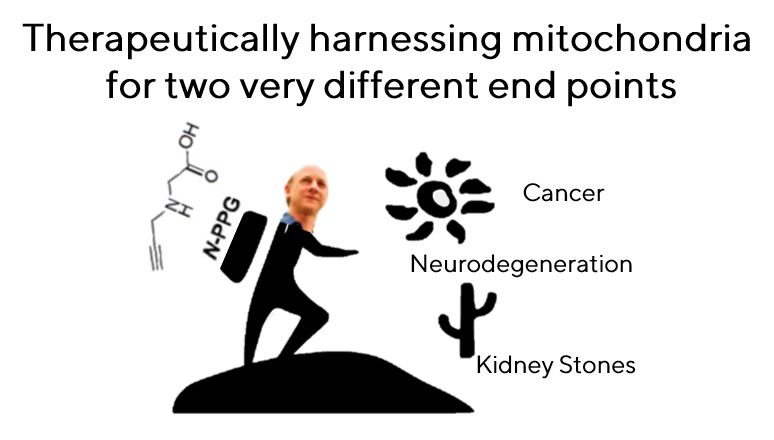
Serendipitous findings lead from a search for anti-cancer agents to a promising treatment for Huntington’s disease… and kidney stones

What happens when an oncologist and a neurobiologist meet in a hallway sounds like it might be the beginning of a bad joke, but it’s actually a story of what new discoveries can be made when differing areas of expertise are combined. A quest that began as a targeted search for a new chemotherapeutic has led to uncovering how it could be used to reduce the symptoms of neurodegenerative diseases. And in a punchline no one saw coming, the drug turns out to be a very promising treatment for kidney stones.
A Chance Encounter Ignites Unexpected Research Trajectories
The genesis of this remarkable scientific journey can be traced back to a simple hallway conversation at the Buck Institute for Research on Aging. Dr. Gary Scott, a senior scientist in the Benz lab, was discussing his work on a mitochondrial enzyme, proline dehydrogenase (PRODH), with Dr. Lisa Ellerby, a Buck Professor. Scott’s lab had been focused on developing novel anti-cancer agents, specifically targeting PRODH with a small molecule inhibitor known as N-propargylglycine (or N-PPG). Their initial investigations, building upon prior Benz lab publications, suggested N-PPG held promise for its ability to impact cancer cells while exhibiting beneficial effects on normal cells.
During their discussion, Scott mentioned that PRODH was implicated in a biological process called "mitohormesis." This phenomenon describes how mild stress within a cell’s mitochondria can actually enhance cellular function and resilience. This specific detail resonated deeply with Dr. Ellerby, whose own research was exploring the role of mitohormesis in neurological diseases.
“When he told me about observing mitohormesis, I thought it was just a perfect match,” Dr. Ellerby recalled. Her lab had been actively investigating the potential therapeutic benefits of inducing mitohormesis in the context of neurodegenerative disorders. Seizing the opportunity, Ellerby proposed a collaborative experiment: testing Scott’s compound, N-PPG, on her Huntington’s disease cell models. This cross-disciplinary inquiry, born from a chance encounter, marked the pivotal moment that would steer their research toward unforeseen and groundbreaking discoveries.
Targeting Neurodegeneration: A Promising Avenue for Huntington’s Disease
Huntington’s disease (HD) is a devastating, inherited neurodegenerative disorder that progressively erodes a person’s physical and mental abilities. It is characterized by involuntary movements (chorea), cognitive decline, and psychiatric disturbances, with no current cure or effective treatment to halt its progression. The disease arises from a genetic mutation that leads to the production of a toxic protein, which gradually damages neurons, particularly in the brain regions controlling movement and cognition.
Motivated by the potential of mitohormesis to combat cellular dysfunction, Dr. Ellerby’s lab initiated experiments with N-PPG on cell lines engineered to model Huntington’s disease. The initial results in cell culture, while encouraging, hinted at something more profound when they moved to a more complex animal model. The team decided to test N-PPG in a mouse model that mimicked severe and rapidly progressing Huntington’s disease. This aggressive model provided a stringent test for any potential therapeutic agent.
A critical early finding was the ability of N-PPG to effectively cross the blood-brain barrier. This is an essential prerequisite for any drug intended to treat neurological conditions, as it allows the therapeutic compound to reach its target within the central nervous system. Furthermore, as anticipated from their earlier studies, the drug demonstrated a lack of discernible toxic side effects, a crucial factor for any potential therapeutic. Most importantly, N-PPG successfully induced mitohormesis in the affected brain cells, as the researchers had hypothesized.
However, the most astonishing discovery emerged from a deeper analysis of the molecular changes occurring in the brains of the treated mice. Dr. Ellerby described the findings as "shocking": N-PPG not only alleviated some of the pathological hallmarks of HD but also significantly corrected the underlying genetic expression patterns associated with the disease. Specifically, the drug reversed the disease-associated transcriptomic changes by approximately 50%.

“We were kind of shocked, like we just gave this drug to the mouse and it was putting the Huntington’s disease brain transcriptomics back toward normal,” Dr. Ellerby stated. “I don’t think we have ever seen a drug that reversed it by that much.”
Dr. Chris Benz, a Buck Professor and a key figure in the Benz lab, emphasized the challenging nature of the model used. “The model we chose was a very difficult one; it is the most aggressive model of Huntington’s disease we have,” he explained. “It is really hard to get something to reverse a pathology when it has already become well established and causing symptoms,” he added, underscoring the significance of their observation.
An Unforeseen Detour: The Promise for Kidney Stone Treatment
The scientific exploration of N-PPG took another unexpected turn when the researchers delved into the metabolic pathways influenced by the drug. Their investigations revealed that N-PPG played a role in the liver’s metabolic pathway responsible for producing oxalate. Oxalate is a key component in the formation of kidney stones, the painful crystallization of minerals in the kidneys. This metabolic insight opened an entirely new and unanticipated avenue of research for the team.
“We became quite excited about that, generating our interest in a completely different field: nephrology,” said Dr. Scott, referring to the branch of medicine dealing with the kidneys.

Dr. Ellerby, whose primary focus is on rare neurological diseases affecting small patient populations, also embraced this new direction. She acquired a mouse model for a rare kidney disease characterized by extensive kidney stone formation. Upon treating these mice with N-PPG, the results were remarkably positive. The drug not only completely cleared the existing kidney stones but also led to a dramatic reduction in oxalate levels within the animals.
This serendipitous discovery, transforming a potential anti-cancer agent into a promising treatment for a common and often debilitating condition, was detailed in a published paper. Dr. Scott noted the use of the word "serendipity" in their publication, aptly describing the nature of their findings.
Dr. Benz reflected on the evolution of their research: “This is not a project I ever would have considered undertaking. I am an oncologist and my lab generally works in the field of cancer and aging. I didn’t envision that it would go in the direction of neurodegeneration and kidney stones but that’s where the data and excitement led us.”
The Power of Interdisciplinary Collaboration at the Buck Institute
The remarkable trajectory of N-PPG from an anti-cancer candidate to a potential therapy for neurodegenerative diseases and kidney stones underscores the profound impact of interdisciplinary collaboration. The Buck Institute for Research on Aging fosters an environment where scientists from diverse fields can readily interact and share expertise, leading to synergistic discoveries.
“It has been a fun collaboration, and it shows what can happen when your next-door neighbor is open and receptive the way Lisa is,” Dr. Scott remarked, highlighting the ease of collaboration within the institute.
Dr. Benz further elaborated on the unique culture at the Buck Institute: “It really attests to a unique quality among the Buck Institute scientists: collaborative and interdisciplinary research, not typically found within larger US academic universities and institutes.” This institutional commitment to breaking down traditional scientific silos has proven instrumental in unlocking novel therapeutic possibilities.
The journey of N-PPG serves as a compelling case study for the power of scientific curiosity, unexpected findings, and the crucial role of collaboration in advancing human health. What began as a targeted search for cancer treatments has blossomed into a multi-faceted research endeavor with the potential to significantly improve the lives of individuals suffering from devastating neurological disorders and the widespread affliction of kidney stones. The ongoing research is expected to delve deeper into the precise mechanisms by which N-PPG exerts its effects, paving the way for potential clinical trials and, ultimately, new therapeutic options for patients. The scientific community will be closely watching as this serendipitous discovery continues to unfold.








{kind=link}