
President Trump’s FY 2027 Budget Request Proposes Significant Cuts to Domestic HIV Programs Amidst Broader Health Policy Shifts.
President Donald Trump’s second-term fiscal year 2027 (FY 2027) budget request, unveiled on April 3, 2026, has ignited significant concern within the public health community, proposing a substantial reduction in funding for numerous domestic HIV programs. This budget blueprint, the second of his current term, delineates the administration’s policy priorities and desired funding levels, often signaling a departure from established federal health initiatives. While presidential budget requests serve as a starting point for congressional appropriations, Congress ultimately holds "the power of the purse," meaning final funding allocations can, and frequently do, diverge from the administration’s proposals. Notably, a similar call for reduced HIV funding in President Trump’s FY 2026 budget request was largely rejected by Congress, which subsequently appropriated funding levels akin to previous years.
The FY 2027 request for domestic HIV programs outlines a sweeping $1.6 billion decline, representing a precipitous 35% cut compared to the final FY 2026 funding levels. This proposed reduction would dismantle or significantly transform several core programs while maintaining others, creating a landscape of uncertainty for HIV prevention, care, and research across the nation. Absent from this budget, as with the FY 2026 request, are proposals to bolster Pre-Exposure Prophylaxis (PrEP) uptake, a cornerstone of HIV prevention strategies championed by the preceding Biden Administration. However, funding for the "Ending the HIV Epidemic Initiative" (EHE), an ambitious effort initiated during the first Trump Administration, has been notably maintained, albeit with significant structural realignments.
A Pattern of Administrative Actions and Uncertainty
Beyond the conventional budget cycle, the Trump administration has previously utilized various executive actions to curtail or terminate already appropriated funding, even for accounts and grants related to HIV. These actions have included delaying or outright canceling funds, leading to considerable uncertainty regarding the availability of federal dollars for HIV programs, grantees, and sub-grantees, even after Congress has formally appropriated them. Such moves have, in some instances, prompted litigation, with states like California successfully suing the administration to protect health funding, sometimes resulting in the reinstatement of critical grants.
Furthermore, the administration has employed the rescission process, a mechanism through which the president asks Congress to cancel appropriated funds. While this process requires congressional approval to reduce funding, it has not yet directly impacted domestic HIV accounts. The cumulative effect of these administrative maneuvers has been a pervasive sense of instability within the public health sector, complicating long-term planning and service delivery for vulnerable populations relying on federal support for HIV care.
Proposed Structural Reorganizations and Program Eliminations
A central feature of the FY 2027 request is the proposed creation of a new agency, the Administration for Healthy America (AHA). This proposal, which Congress rejected in the FY 2026 appropriations process, seeks to consolidate key health programs currently housed within other agencies. Under this plan, the Ryan White HIV/AIDS and Health Center Programs, traditionally under the Health Resources and Services Administration (HRSA), would be transferred to AHA. The budget narrative asserts that AHA would prioritize HIV/AIDS programs, aligning with the administration’s broader health priorities. This consolidation would also encompass funding for the Office of Infectious Disease and HIV/AIDS Policy (OIDP) and all EHE funding previously allocated to the Centers for Disease Control and Prevention (CDC).

Simultaneously, the budget request calls for the outright elimination of several long-standing and critical HIV programs. This includes core domestic HIV prevention funding at the CDC, which historically accounts for nearly 91% of federal funding for domestic HIV prevention. Part F of the Ryan White HIV/AIDS Program, a component dedicated to specific support services, is also slated for elimination. Significant portions of the Minority AIDS Initiative (MAI), designed to address the disproportionate impact of HIV on racial and ethnic minority communities, would also be cut or eliminated. Furthermore, the National Institute of Allergy and Infectious Diseases (NIAID) at the National Institutes of Health (NIH), the world’s largest source of HIV research funding, faces substantial cuts. The Housing Opportunities for Persons with AIDS (HOPWA) program, administered by the Department of Housing and Urban Development (HUD), is also targeted for elimination, a move that would critically impact housing stability for low-income individuals living with HIV.
Detailed Program-Specific Impacts
Centers for Disease Control and Prevention (CDC) – Domestic HIV Prevention: The budget request proposes the complete elimination of funding for core HIV prevention programs at the CDC. The only HIV-related funding preserved, $220 million for EHE activities, would be transferred from the CDC to the proposed AHA. This represents a staggering $794 million decrease, or a 78% cut, from the FY 2026 level of $1 billion (which included EHE funding), effectively eliminating the CDC’s dedicated HIV prevention division. While HIV prevention funds are cut, some infectious disease funding is retained and grouped into a single $300 million account, combining previously separate lines for viral hepatitis, sexually transmitted infections, and tuberculosis prevention. This consolidated amount is $70 million below the sum of the individual accounts in FY 2026. These proposed changes at the CDC mirror those in the FY 2026 budget request, which Congress ultimately rejected.
Ryan White HIV/AIDS Program: The Ryan White HIV/AIDS Program, a crucial safety-net for HIV care and treatment in the U.S., currently housed at HRSA and proposed for transfer to AHA, is slated to receive $2.5 billion in the FY 2027 request. This represents a $74 million (3%) decrease from the FY 2026 enacted level. The request includes $165 million for EHE activities within Ryan White, maintaining the FY 2026 level. The overall reduction is attributed to the elimination of funding for Part F of the program, which encompasses specific support components. The Health Center Program, also proposed for transfer to AHA, would receive $157 million in HIV funding, entirely dedicated to the EHE initiative, consistent with FY 2026 levels. This funding supports outreach, testing, and increased access to PrEP for patients.
Office of Infectious Disease and HIV/AIDS Policy (OIDP): The FY 2027 budget allocates $7.6 million to OIDP, currently under the Office of the Assistant Secretary for Health and proposed for transfer to AHA. OIDP plays a vital coordinating role, including for EHE efforts and national strategies for HIV, STIs, and viral hepatitis. The funding aims to "drive progress [in] AHA priorities by implementing innovative, evidence-based interventions to prevent, diagnose, and treat HIV/AIDS, STIs, viral hepatitis, nosocomial infections/hospital – acquired infections (HAIs), and antibiotic-resistant organisms," as well as supporting national strategies and community engagement.
National Institutes of Health (NIH) – Domestic HIV Research: The NIH has historically been the primary federal entity conducting HIV research. The budget proposes substantial cuts to NIH overall, with the National Institute of Allergy and Infectious Disease (NIAID) facing a $1.8 billion (27%) reduction, from approximately $6.5 billion to $4.8 billion. While the precise allocation for domestic HIV research at NIH in FY 2027 is not yet known, it stood at $3.3 billion in FY 2025. The Office of AIDS Research (OAR), located within the Office of the NIH Director, which coordinates HIV research across NIH, is mentioned in the budget’s technical appendix, though a specific funding amount is not provided. Such deep cuts to NIAID could severely impede progress in vaccine development, new treatment modalities, and basic science understanding of HIV.
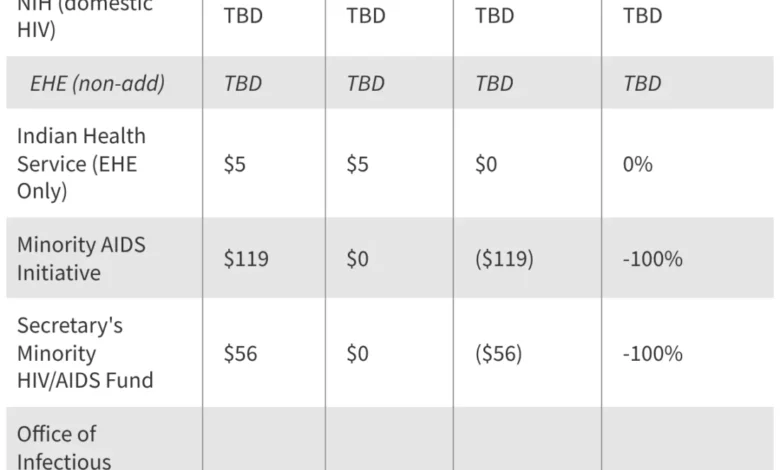
Indian Health Service (IHS): The FY 2027 budget continues $5 million for IHS EHE activities, aimed at supporting efforts to end HIV and hepatitis C in Indian Country, consistent with the FY 2026 final level. This funding is critical for addressing the unique health disparities faced by Native American communities.
The Minority AIDS Initiative (MAI): Created in 1998, the MAI was designed to address the disproportionate impact of HIV on racial and ethnic minority communities and build organizational capacity within them. The status of MAI funding under the FY 2027 request is largely uncertain. Funding for MAI activities at the Substance Abuse and Mental Health Services Administration (SAMHSA), aimed at improving the health of people of color affected by or at risk for HIV, is eliminated in the proposal. In FY 2026, SAMHSA received $119 million for MAI. An additional $56 million in MAI funding from the Secretary’s Minority HIV/AIDS account is also eliminated. Furthermore, the elimination of Ryan White Part F, which includes an MAI funding line, contributes to the overall decimation of this critical initiative.
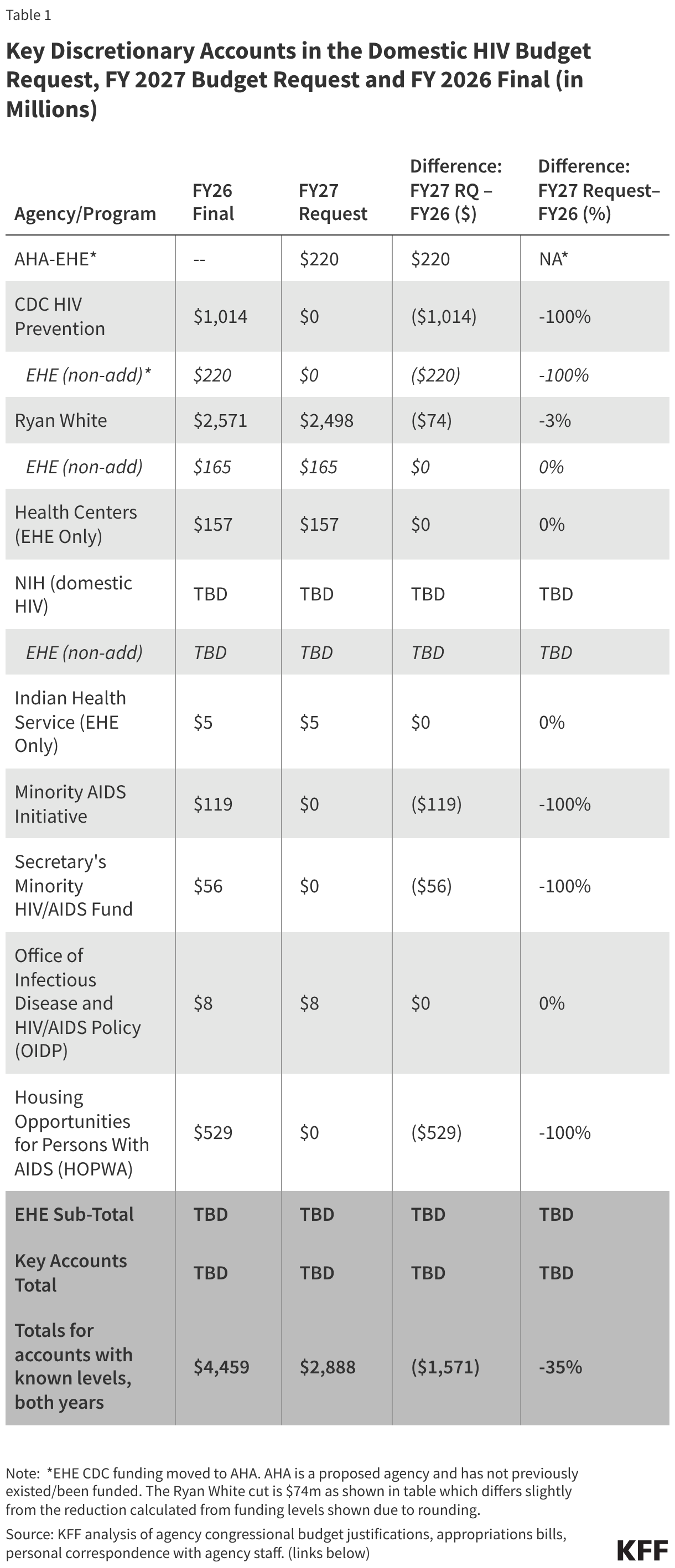
Housing Opportunities for Persons with AIDS (HOPWA): The Department of Housing and Urban Development’s (HUD) HOPWA Program, a cornerstone of support for low-income people with HIV facing housing insecurity, is entirely eliminated in the budget request. In FY 2026, HOPWA was funded at $529 million. Established in 1992, HOPWA is the only federal program specifically dedicated to the housing needs of people with HIV, providing grants to localities, states, and community-based organizations. Its elimination would leave countless individuals vulnerable to homelessness, which is a significant barrier to consistent HIV treatment and prevention.
Broader Policy Landscape and Implications
These proposed cuts arrive at a precarious time when other changes to the health policy landscape could further jeopardize access to HIV care and prevention services. Recent federal budget reconciliation laws have included provisions related to Medicaid work requirements, which could restrict access for eligible individuals living with HIV. The potential expiration of premium tax credits under the Affordable Care Act (ACA) could also impact affordability of health insurance for many people with HIV. Furthermore, constrained state budgets have already led some states to restrict HIV drug access through the Ryan White program, and access to newer prevention tools like injectable PrEP remains uncertain. The cumulative effect of these proposed cuts and broader policy shifts could significantly undermine decades of progress in combating the HIV epidemic in the United States.
Public health advocates and patient organizations are expected to voice strong opposition to these proposed reductions, emphasizing the potential for increased HIV transmissions, poorer health outcomes, and exacerbated health disparities, particularly among minority populations and those in underserved communities. Concerns would likely be raised about the long-term economic costs of failing to invest in prevention and care, arguing that cuts now could lead to higher healthcare expenditures in the future.
The Road Ahead: Congressional Scrutiny
As in previous years, the presidential budget request serves as a policy statement rather than a definitive financial blueprint. The ultimate decision on funding levels for these critical HIV programs rests with Congress. Given the bipartisan support for many HIV initiatives in the past, and Congress’s previous rejection of similar proposed cuts, it is anticipated that lawmakers will thoroughly scrutinize these proposals. Advocacy groups and public health organizations will undoubtedly engage in robust lobbying efforts to highlight the vital importance of sustained federal investment in HIV prevention, treatment, and research. The coming months will be crucial in determining whether the proposed cuts become reality or if Congress once again asserts its "power of the purse" to protect and preserve essential services for people living with or at risk for HIV. The tables provided illustrate the stark contrast between the FY 2027 budget request and the FY 2026 enacted levels for key discretionary accounts in domestic HIV funding, including a dedicated breakdown for EHE funding, underscoring the magnitude of the proposed changes.






{kind=link}