
Breathing Irregularities and Dysfunctional Respiration Patterns Identified as Major Factors in Chronic Fatigue Syndrome Symptoms
The medical community has long struggled to pinpoint the underlying physiological mechanisms of Myalgic Encephalomyelitis, commonly known as Chronic Fatigue Syndrome (ME/CFS). This debilitating condition, which affects millions of individuals globally, is characterized by profound exhaustion, cognitive impairment, and a hallmark symptom known as post-exertional malaise (PEM)—the worsening of symptoms following even minor physical or mental activity. However, a groundbreaking study from the Icahn School of Medicine at Mount Sinai has identified a significant, previously overlooked factor: a high prevalence of dysfunctional breathing and hyperventilation among CFS patients. Published in the journal Frontiers in Medicine, the research suggests that these respiratory irregularities may not only contribute to the severity of the disease but could also offer a new pathway for therapeutic intervention.
The study, led by senior author Dr. Benjamin Natelson and first author Dr. Donna Mancini, reveals that nearly half of the chronic fatigue subjects examined exhibited some form of breathing disorder. This finding provides a tangible physiological marker for a condition that has historically been difficult to diagnose and treat. By shifting the focus toward the respiratory system and its interaction with the autonomic nervous system, researchers believe they can develop strategies to alleviate some of the most burdensome symptoms of the syndrome, such as shortness of breath, dizziness, and "brain fog."
The Scope and Methodology of the Mount Sinai Study
To investigate the relationship between respiration and CFS, the research team at Icahn Mount Sinai conducted a rigorous comparative analysis. The study cohort consisted of 57 individuals diagnosed with chronic fatigue syndrome and a control group of 25 healthy individuals. To ensure the accuracy of the comparison, the control group was matched for age and general activity levels.
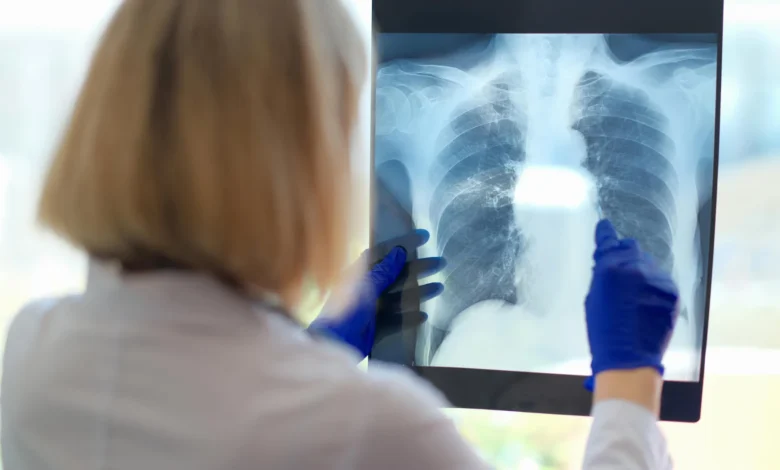
The core of the research involved a two-day protocol of cardiopulmonary exercise tests (CPET). This two-day approach is particularly significant in CFS research; while a single exercise test might not show abnormalities in CFS patients, the second day of testing often captures the physiological "crash" associated with post-exertional malaise. During these sessions, participants were monitored for a wide array of physiological metrics, including heart rate, blood pressure, oxygen uptake efficiency, and blood oxygen saturation.
Crucially, the researchers also analyzed the mechanics of breathing. They monitored how much effort participants exerted to breathe and tracked breathing rates to detect signs of hyperventilation and dysfunctional breathing. Hyperventilation involves breathing that is too rapid or deep, leading to a drop in carbon dioxide levels in the blood, whereas dysfunctional breathing refers to irregular patterns that do not meet the body’s metabolic needs efficiently.
Defining Dysfunctional Breathing in the Context of Chronic Illness
Dysfunctional breathing (DB) is a term often associated with respiratory conditions like asthma, yet it can manifest in various ways across different pathologies. It is fundamentally a biomechanical issue where the muscles used for respiration do not work in a coordinated or efficient manner.
Common features of dysfunctional breathing identified in the study include:
- Frequent deep sighing.
- Rapid, shallow breathing.
- Forceful exhalation involving the abdominal muscles.
- "Chest breathing," where the upper chest does most of the work rather than the diaphragm.
- A lack of coordination between the chest and abdomen, preventing the lungs from expanding to their full capacity.
Dr. Donna Mancini noted that while the medical community understands the symptoms of hyperventilation—such as tingling in the extremities and lightheadedness—the specific impact of dysfunctional breathing on CFS patients remains an area of active discovery. Significantly, many patients are entirely unaware that their breathing patterns are irregular, as these patterns can persist even when the patient is in a resting state.
Comparative Data: CFS Patients vs. Healthy Controls
The results of the study were stark, highlighting a clear divergence between the CFS group and the healthy controls. While both groups showed similar "peak VO2 max" levels—meaning their basic capacity to take in and use oxygen during peak exertion was roughly the same—the way they reached that peak differed significantly.
The data revealed that 71% of the chronic fatigue group exhibited some form of breathing abnormality. When broken down further, the results showed:
- Irregular Breathing: Nearly 50% of the CFS participants breathed irregularly during the tests, compared to only 16% (four individuals) in the healthy control group.
- Hyperventilation: Approximately one-third of the CFS patients hyperventilated during the sessions, while only 4% (one individual) of the control group did.
- Combined Disorders: Nine patients in the CFS group suffered from both hyperventilation and dysfunctional breathing simultaneously. This combination was not observed in any member of the control group.
These findings suggest that for many CFS patients, the feeling of "air hunger" or shortness of breath is not a result of lung damage or low fitness, but rather a failure of the respiratory control system.
The Role of Dysautonomia and the Autonomic Nervous System
The researchers posit that the root cause of these breathing irregularities may lie in dysautonomia—a disorder of the autonomic nervous system (ANS). The ANS controls involuntary bodily functions, including heart rate, blood pressure, and digestion. In many CFS patients, the ANS does not function correctly, a condition often manifesting as orthostatic intolerance (feeling worse when standing up).
Dr. Mancini explained that dysautonomia could trigger rapid and irregular breathing. When a patient with orthostatic intolerance stands, their heart rate may spike, and their body may enter a "fight or flight" state, leading to hyperventilation. This physiological stressor can exacerbate the exhaustion and cognitive difficulties that define the CFS experience. The link between the nervous system and the lungs suggests that CFS is a multi-systemic disorder rather than a localized one.
Historical Context and the Search for Biomarkers
For decades, patients with chronic fatigue syndrome faced skepticism from the medical establishment, with many symptoms dismissed as psychosomatic. It was not until 2015 that the Institute of Medicine (now the National Academy of Medicine) redefined ME/CFS as a serious, systemic, and chronic disease. Despite this recognition, the lack of a definitive "blood test" or biomarker has made diagnosis a process of exclusion.
This study adds to a growing body of evidence seeking to establish objective physiological markers for the disease. By quantifying breathing irregularities, the Mount Sinai team has provided a measurable metric that clinicians can use to assess the severity of a patient’s condition. This follows other recent research into mitochondrial dysfunction and gut microbiome imbalances, all of which point to a complex, systemic failure in CFS patients.
Implications for Treatment: Pulmonary Physiotherapy and Biofeedback
The identification of breathing disorders in CFS patients opens the door to specialized treatments that have previously been underutilized in this population. While traditional "graded exercise therapy" has been controversial and often harmful to CFS patients due to the risk of PEM, targeted breathing exercises may offer a safer alternative.
Dr. Natelson suggested several potential avenues for treatment:
- Yoga and Breath Control: Gentle yoga focused on pranayama (breath control) could help retrain the diaphragm and reduce reliance on chest breathing.
- Biofeedback: Utilizing devices that measure exhaled carbon dioxide (CO2) can provide patients with real-time data. If a patient sees that their CO2 levels are low—a sign of hyperventilation—they can consciously work to slow their breathing and raise those levels to a normal range.
- Pulmonary Physiotherapy: Specialized physical therapy that focuses on the mechanics of the ribs and diaphragm may help restore coordination between the chest and abdominal muscles.
- Swimming: Because swimming requires rhythmic, controlled breathing, it may serve as a gentle form of physical conditioning that supports respiratory health without triggering the severe crashes associated with high-impact exercise.
Analysis of Broader Impacts
The findings of this study have implications beyond the immediate CFS community. With the rise of Long COVID, which shares many clinical features with ME/CFS, the discovery of dysfunctional breathing patterns may provide a roadmap for treating the millions of people currently suffering from post-viral fatigue. Many Long COVID "long-haulers" report persistent shortness of breath despite having clear lung scans; the Mount Sinai study suggests that their issue may also be one of respiratory mechanics and autonomic control.
Furthermore, the study underscores the necessity of a multidisciplinary approach to chronic illness. When researchers from neurology, cardiology, and pulmonology collaborate, they can uncover "unappreciated issues" that a single-specialty focus might miss. As Dr. Natelson concluded, the ultimate goal is to reduce the symptom burden for patients who have long been left without answers.
By identifying that nearly three-quarters of CFS patients suffer from breathing abnormalities, this research provides a new lens through which to view the disease. It moves the conversation away from vague "fatigue" and toward specific, treatable physiological dysfunctions. As further studies validate these findings, breathing assessment may become a standard part of the diagnostic workup for anyone presenting with chronic, unexplained exhaustion.




{kind=link}