
United States Bolsters Global Health Initiatives Across Over 80 Nations in FY 2024, Addressing Critical Health Challenges Worldwide
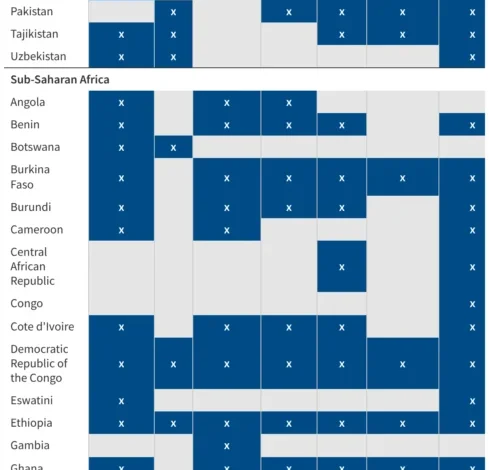
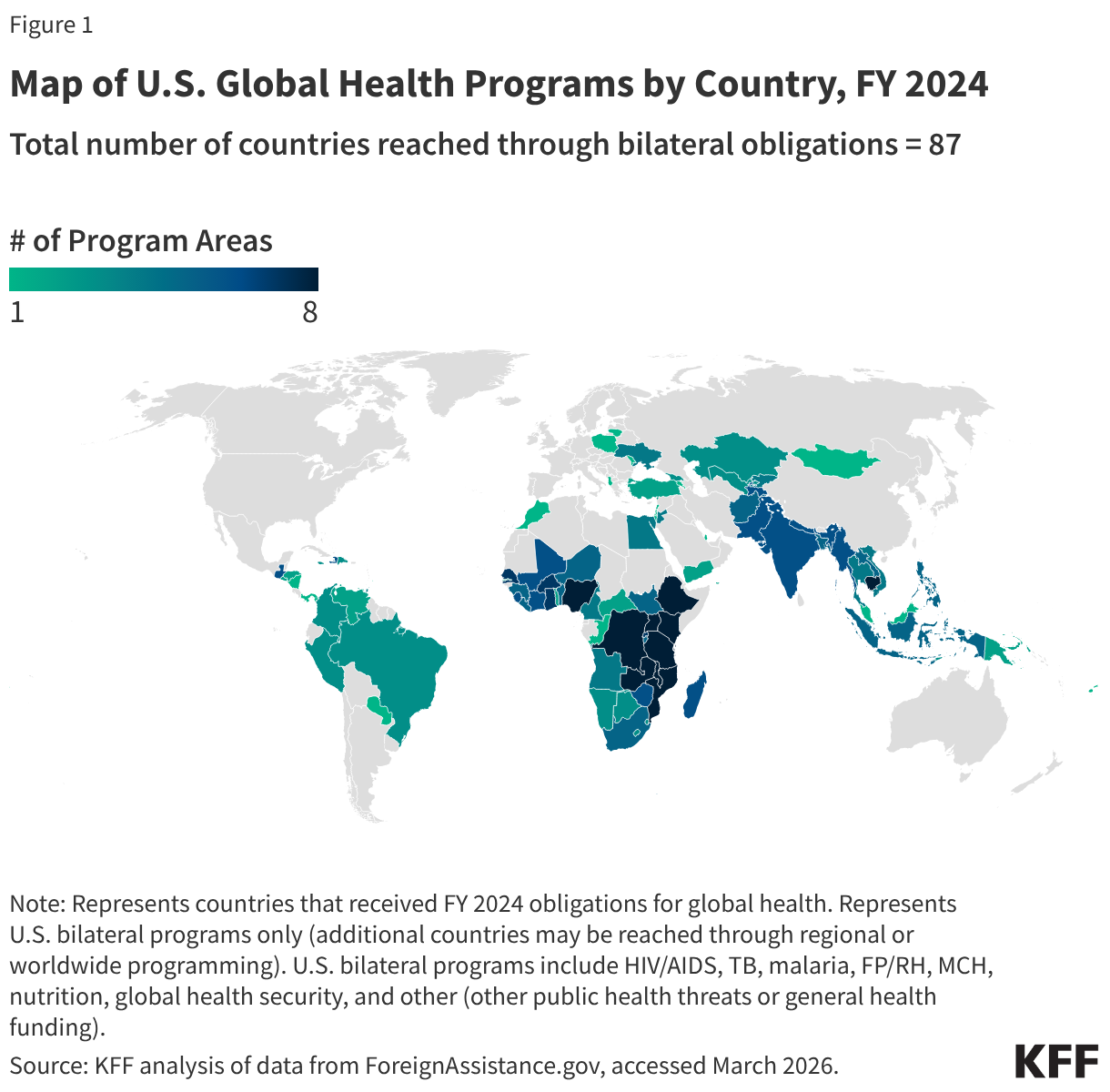
The United States continues its extensive commitment to global health, supporting comprehensive programs in over 80 countries as reflected in Fiscal Year 2024 data. This vast network of initiatives extends its reach further through regional efforts and substantial contributions to multilateral organizations, underscoring America’s enduring role as a leading force in international public health. U.S. programs in partner nations are multifaceted, often encompassing a diverse array of critical health areas. These include the globally renowned President’s Emergency Plan for AIDS Relief (PEPFAR), robust efforts against Tuberculosis (TB), the impactful President’s Malaria Initiative (PMI), vital Family Planning and Reproductive Health (FP/RH) services, foundational Maternal and Child Health (MCH) interventions, crucial Nutrition programs, and paramount Global Health Security initiatives. This strategic and widespread engagement is meticulously tracked to provide an overview of U.S. bilateral global health programs by country and region, ensuring transparency and accountability in its far-reaching efforts.
The Genesis of U.S. Global Health Engagement: A Historical Perspective
America’s involvement in global health is not a recent phenomenon but rather a commitment that has evolved significantly over decades, rooted in both humanitarian principles and strategic interests. The establishment of the U.S. Agency for International Development (USAID) in 1961 marked a formalization of foreign assistance, with health aid quickly becoming a cornerstone. Early efforts often focused on basic sanitation, disease control, and vaccine campaigns. However, the late 20th and early 21st centuries witnessed a dramatic scaling up and refocusing of these efforts, driven by emerging global health crises and a recognition of health as a critical component of national security and economic development.
A pivotal moment arrived in 2003 with the launch of PEPFAR by President George W. Bush. This groundbreaking initiative fundamentally transformed the global response to HIV/AIDS, providing unprecedented funding and support for prevention, treatment, and care in the hardest-hit regions, particularly sub-Saharan Africa. Prior to PEPFAR, HIV/AIDS was decimating populations, shattering economies, and creating widespread social instability. Its creation signaled a new era of large-scale, disease-specific global health intervention. Following PEPFAR’s success, the President’s Malaria Initiative (PMI) was launched in 2005, targeting another devastating infectious disease, initially in a subset of African countries, before expanding its geographic scope and programmatic interventions. These flagship programs laid the groundwork for a more integrated and comprehensive approach to global health challenges. The experience gained from these initiatives also highlighted the importance of strengthening local health systems, fostering sustainable solutions, and building local capacity – principles that now underpin much of U.S. global health strategy.
Key Pillars of Support: Program Areas in Detail
The current suite of U.S. global health programs, as reflected in FY 2024 data, represents a sophisticated and integrated approach to complex health challenges. Each program area addresses specific needs while often contributing to the overall strengthening of national health systems.
PEPFAR (President’s Emergency Plan for AIDS Relief): Since its inception, PEPFAR has been one of the most successful foreign assistance programs in history, responsible for saving millions of lives and fundamentally altering the trajectory of the global HIV/AIDS epidemic. It supports antiretroviral treatment for millions, prevents mother-to-child transmission, provides care for orphans and vulnerable children, and implements prevention strategies. As of its latest reporting, PEPFAR has supported over 20 million people with life-saving antiretroviral treatment. Its focus has evolved from emergency response to achieving epidemic control, emphasizing sustainability, local ownership, and efficient resource allocation. The program also plays a crucial role in strengthening health systems, laboratories, and supply chains, which have proven invaluable in responding to other health crises, including the COVID-19 pandemic.
Tuberculosis (TB): The U.S. is a major contributor to global efforts to combat TB, a preventable and curable disease that remains one of the world’s deadliest infectious killers. U.S. programs focus on improving diagnosis and treatment rates, particularly for drug-resistant TB, strengthening laboratory networks, and supporting research into new diagnostics, drugs, and vaccines. These efforts are often aligned with the World Health Organization’s (WHO) End TB Strategy, aiming to reduce TB incidence and deaths globally.
President’s Malaria Initiative (PMI): PMI is a testament to the power of targeted intervention. It works to reduce malaria-related deaths and illness in dozens of countries, primarily in sub-Saharan Africa and the Greater Mekong Subregion. Key interventions include the distribution of insecticide-treated bed nets, indoor residual spraying, improved diagnostics, and access to effective antimalarial treatments. PMI’s rigorous, evidence-based approach has contributed to significant declines in malaria prevalence and mortality in partner countries, protecting millions from the disease.
Family Planning and Reproductive Health (FP/RH): U.S. support for FP/RH programs empowers individuals and couples to make informed decisions about family size and spacing, leading to healthier families and communities. These programs provide access to a range of contraceptive methods, counseling, and related reproductive health services. Investing in FP/RH is recognized as a cost-effective intervention that improves maternal and child health outcomes, promotes gender equality, and contributes to economic development.
Maternal and Child Health (MCH): The U.S. is deeply committed to reducing preventable maternal and child deaths, particularly in low-resource settings. MCH programs encompass a wide range of interventions, including skilled birth attendance, postnatal care, childhood immunizations, nutrition support for pregnant women and young children, and treatment for common childhood illnesses like pneumonia and diarrhea. These programs are often integrated with other health services to provide comprehensive care.
Nutrition: Malnutrition remains a fundamental cause of child mortality and hinders physical and cognitive development. U.S. nutrition programs address various forms of malnutrition, from stunting and wasting in children to micronutrient deficiencies. Interventions include promoting exclusive breastfeeding, providing micronutrient supplements, supporting therapeutic feeding programs, and improving food security through agricultural development and resilience-building efforts.
Global Health Security (GHS): The COVID-19 pandemic starkly highlighted the interconnectedness of global health and the imperative of robust global health security. U.S. GHS initiatives focus on strengthening countries’ capacities to prevent, detect, and respond to infectious disease threats, whether naturally occurring, accidental, or deliberate. This involves building surveillance systems, laboratory capacity, emergency preparedness and response capabilities, and workforce development, often guided by the Global Health Security Agenda (GHSA) framework.
Geographic Reach and Strategic Partnerships
The U.S. global health footprint in FY 2024 extends across a remarkably diverse geographic landscape, covering over 80 direct bilateral partner countries. This extensive reach is strategically important, allowing the U.S. to address health disparities in regions most affected by disease burdens and to build resilient health systems where they are most needed. While specific countries vary based on programmatic focus and evolving needs, the concentration often includes nations in sub-Saharan Africa, Southeast Asia, Latin America, and Eastern Europe, areas historically impacted by infectious diseases and with significant development challenges.
Beyond direct bilateral aid, the U.S. amplifies its impact through significant contributions to multilateral organizations. These include the World Health Organization (WHO), the Global Fund to Fight AIDS, Tuberculosis and Malaria, Gavi, the Vaccine Alliance, and UNICEF, among others. By supporting these global platforms, the U.S. leverages collective expertise and resources, ensuring broader coverage and coordinated global responses to health crises. This dual approach of bilateral engagement and multilateral partnership maximizes the efficiency and effectiveness of U.S. global health investments, fostering a collaborative environment critical for addressing cross-border health threats.
Funding Landscape and Impact Metrics
U.S. global health funding represents a substantial investment of taxpayer dollars, consistently ranking among the largest contributions from any single nation. While the specific figures for FY 2024 bilateral global health funding are tracked and publicly available through resources like the KFF U.S. global health country-level funding tracker, historical trends indicate annual commitments often exceeding $10 billion, depending on the precise definition of "global health" aid. This funding is meticulously allocated across the various program areas, with significant portions dedicated to PEPFAR and PMI due to their scale and established impact.
The tangible results of these investments are profound. For instance, PEPFAR has been credited with saving over 25 million lives globally and fundamentally transforming the HIV/AIDS epidemic from a death sentence to a manageable chronic condition in many regions. PMI has contributed to a dramatic reduction in malaria cases and deaths in its focus countries. MCH and nutrition programs have led to decreases in maternal and child mortality rates, improved child survival, and healthier populations capable of contributing to their nations’ economic growth. Global Health Security initiatives, while harder to quantify in terms of lives saved from averted pandemics, represent a critical investment in proactive defense against future health crises, providing foundational capabilities that strengthen national and international resilience. The emphasis on data-driven programming, monitoring, and evaluation ensures that these funds are utilized effectively and transparently, maximizing their health impact.
Statements from Officials and Stakeholders
While the original data does not include direct quotations, the consistent nature and scale of U.S. global health funding in FY 2024 allow for logical inference regarding official U.S. government stances and reactions from partner nations and the international health community.
A U.S. official, perhaps the Secretary of State or the Administrator of USAID, would likely reiterate the nation’s unwavering commitment to global health. Such a statement might emphasize: "Our investment in global health is not merely an act of generosity; it is a strategic imperative. Healthy populations are more stable, more prosperous, and better equipped to contribute to global security. The extensive reach of our programs in FY 2024, from battling AIDS and malaria to strengthening health systems and preparing for future pandemics, reflects our conviction that America’s health and security are inextricably linked to the health and security of people worldwide. We are proud of the millions of lives saved and improved through these partnerships."
From the perspective of a partner country’s Ministry of Health, there would likely be expressions of gratitude and acknowledgment of the tangible benefits. A representative might state: "The sustained support from the United States, particularly through initiatives like PEPFAR and PMI, has been transformative for our nation. It has enabled us to provide life-saving treatments, protect our children from preventable diseases, and build the capacity of our health workforce. This partnership is vital in our ongoing efforts to achieve universal health coverage and ensure a healthier future for our citizens."

Moreover, leading global health organizations and non-governmental organizations (NGOs) would likely commend the U.S. for its consistent leadership and financial contributions. An NGO executive might comment: "The breadth and depth of U.S. global health programming, as demonstrated in the FY 2024 data, remain unparalleled. This commitment is the bedrock upon which much of the global health architecture is built, allowing for coordinated responses to complex challenges and fostering innovation that benefits us all."
Challenges, Opportunities, and the Future of U.S. Global Health
Despite the significant achievements, the landscape of global health is dynamic and fraught with ongoing challenges. Sustained funding remains a perennial concern, as political shifts and economic pressures can impact aid budgets. Emerging threats, such as antimicrobial resistance (AMR), the health impacts of climate change, and the persistent risk of new pandemics, demand continuous adaptation and innovation. Ensuring equity in health service delivery, addressing the needs of marginalized populations, and strengthening local ownership and sustainability are also critical areas of focus. The transition of successful programs from external support to domestically financed systems in partner countries is a complex but necessary long-term goal.
However, these challenges also present immense opportunities. Advances in technology, from digital health solutions and telemedicine to innovative diagnostics and vaccine development, offer new tools to overcome traditional barriers to health access. The lessons learned from the COVID-19 pandemic have galvanized international cooperation and highlighted the urgency of investing in pandemic preparedness and response capabilities, reinforcing the Global Health Security agenda. There is also a growing recognition of the interconnectedness of health with other development sectors, such as education, economic empowerment, and climate resilience, paving the way for more integrated and holistic interventions.
The U.S. commitment to global health, as evidenced by its FY 2024 programming across over 80 countries and myriad health areas, demonstrates a continued dedication to global well-being and security. Looking ahead, the effectiveness of these initiatives will depend on sustained political will, adaptive strategies, robust partnerships, and a relentless focus on evidence-based approaches to achieve lasting impact and foster a healthier, more secure world for all.







{kind=link}